Our research shows that higher Bone Mineral Density (BMD) was associated with a greater risk of fracture, which is opposite of what we would expect. When we picked apart the BMD ratio we found that bone size had the strongest association with fracture risk, such that smaller bones had a greater risk.
This comprehensive review of the research evidence surrounding supportive stepping for individuals, GMFCS IV and V, provides helpful information for families to make practical decisions about for whom, when, and how long to use a supported stepping device (also known as gait trainers).
This comprehensive review of the research evidence surrounding supportive standing for individuals, GMFCS IV and V, provides helpful information for families to make practical decisions about for whom, when, and how long to use a standing device.
NCART Standing Device Funding Guide contains all the information needed to choose, measure, and write a letter of medical necessity for a standing device.

Standing devices and standing wheelchair devices are frequently prescribed and often denied equipment options for individuals with cerebral palsy. The attached paper provides evidence and guidance to help appeal to insurers for this equipment.

Complex Rehabilitation Technology serves to enhance the lives of individuals who utilize it with the goals of maximizing health, wellbeing, participation and independence.

RESNA (Rehab Engineering and Assistive Technology Society of North America) is a great place to find highly qualified rehab and assistive technology professionals in your area. They also have provided their research to help providers and the families they serve make decisions about powered mobility for young children.
Jen Lyman provides a parent perspective on powered wheelchair standing devices as it relates to Dr. Lisa Kenyon's research article.

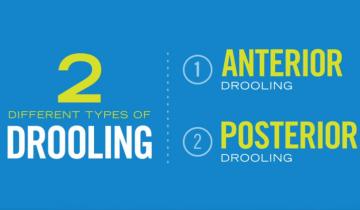
Drooling is an important problem for many individuals with CP and there are a number of interventions available to treat symptoms. If an individual with CP or their caregiver have concerns about drooling it is important to discuss with a health care provider. Care pathways such as the AACPDM pathway can be a starting point for shared decision making. In all cases, working together as a team is important in choosing the best alternative. Children and adults with CP may have trouble with drooling, or saliva management. In the medical world, drooling is referred to as sialorrhea. Saliva plays an important role in eating but also can interfere with airway clearance and breathing, as well as social participation. When drooling has this kind of impact it becomes important to consider intervention.

Many children with cerebral palsy (CP) have difficulty controlling saliva. Drooling varies in severity and can be distressing for the children, families and caregivers. Chronic drooling is referred to as Sialorrhea and occurs as a result of limitations in a person’s ability to control and swallow oral secretions.
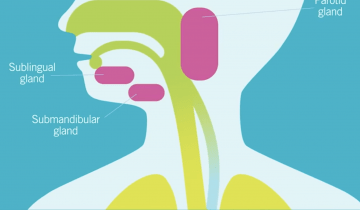
Oropharyngeal dysphagia, or OPD, is an impairment of the oral or pharyngeal phases of the swallow. This can impair muscle movements and coordination of the mouth, such as the lips, tongue, jaw, cheeks, palate, and also muscles of the pharynx and the entry to the airway.

Weight, height and body composition are important indicators for development. The tools used to measure these can be different for children with cerebral palsy.

Children with cerebral palsy (CP) often grow poorly and assessment of growth in this population is further complicated by two main difficulties. Firstly, children may have joint contractures, muscular weakness, scoliosis, and/or involuntary movements that make standing or lying straight difficult, if not impossible.
When we have a physical disability, our bones can get a bit weak or osteoporotic. Something that can be improved is promoting bone health for people with cerebral palsy.