This systematic review looks at all available evidence for pharmacological/neurosurgical interventions for managing dystonia in individuals with cerebral palsy to inform the AACPDM care pathway.
Adults with Cerebral Palsy have unique care needs related to physiological changes that occurred with growth and development with Cerebral Palsy, including mental health, yet experience many barriers to proper care.
We got the diagnosis of Cerebral Palsy when Lelia was 18 months. I was really happy, as we didn’t know what was wrong with her before then. She had low tone. She couldn’t roll over. She couldn’t sit up. Of course she didn’t walk. The diagnosis gave it a name, something I could work with, and I became a kind of vigilante mother, determined to get the best care for my daughter.

The second Virtual Town Hall featured the experts from Rady Children's Hospital, Southern Family CP Center, and UC San Diego School of Medicine in San Diego, California. This multi-disciplinary panel discussion highlights the latest updates in care of children with CerebralPalsy.
Children with cerebral palsy have more complex self-management and self-care demands than children who are typically developing. They have to learn how to deal with medications and they may have to deal with medical equipment. At some point, they're going to have to learn about medical appointments.

There are so many different causes for potential pain that it can be hard to find the cause. If you have CP or are a parent of someone with CP it is really important to empower yourself with information on pain including what causes it and options for treatment. You need to work out what is causing the pain not just mask it with pain medication.

There are a couple of key things to think about in helping children and adolescents make the transition into young adulthood and independence. One of those things is called mastery motivation and we can see mastery motivation early in life. It's the ability to persist in the face of challenge. If you're growing up with a disability, it can be harder to do things. If you are not challenged, if the environment is not set up correctly, or if you don't have the resources, then you start to feel that you can't master certain kinds of tasks.

When we have a physical disability, our bones can get a bit weak or osteoporotic. Something that can be improved is promoting bone health for people with cerebral palsy.

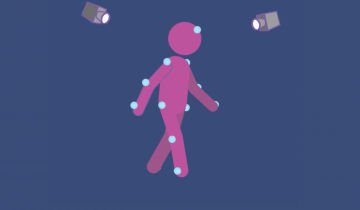
It's really hard just to watch someone walk to decide what's wrong with them. A better way is to do what's called Three Dimensional Gait Analysis, and that's where the child comes into one of our labs. Here, we put markers on their face, hands, and legs. We have a computer and a bunch of cameras all around the room. And then we're able to break down the gait into three dimensions.
Every educator needs to make a decision about technology they need to put in place. They're not sure if they should put Option A in place or Option B in place. This can be particularly difficult in the world of disabilities because there might not always be a perfect answer. Teachers can look to this solution, using the least dangerous assumption to make good decisions about what technology might be best.
It is important to understand the brain injury for each individual person, because they can be really different. Where the injury is can give us important clues to what motor problems that individual will have. The time you have the biggest risk to having a stroke is as a baby, not as an adult so it is important to understand what may be happening in the infants brain.
As an orthopedic surgeon I take care of children from the time they're born all the way through to adulthood . My oldest patient I have is 87 years old. As part of my practice I'm able to take care of all of their musculoskeletal problems, their problems with their bones and their joints.

When you don't have enough evidence about a student's performance, assume they can do whatever you're asking them to do.