Gait Patterns in Cerebral Palsy Fact Sheet
Individuals with cerebral palsy may have a combination of neurological and musculoskeletal issues including balance, sensation, muscle tone, and abnormal movements which can challenge their walking ability and can lead to additional wear and tear on the bones and joints over time.
Although people might have similar walking patterns, the way their muscles and joints work together can vary widely. This is particularly true in people with cerebral palsy. Understanding different gait patterns is important because it can determine what interventions will potentially be the most effective. For people who have cerebral palsy, treatments to improve or maintain walking function typically include measures to reduce high muscle tone. It can also include orthopedic surgery to correct bony deformities, balance muscles and improve joint function.
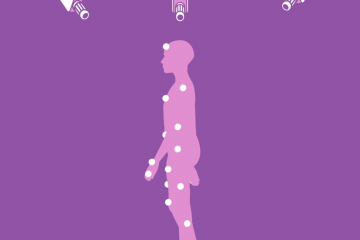
The best way to assess gait patterns is with gait and motion analysis. The main components of gait and motion analysis include an observational video, a musculoskeletal examination, a thorough survey of functional status and, finally, instrumented three-dimensional motion analysis. Three-dimensional motion analysis is a complex process involving the use of a number of technologies including: high-resolution motion tracking cameras, reflective markers, electromyography, ground reaction force plates and pedo-barography.
Along with a cardiorespiratory metabolic measurement system, the equipment measures:
• Motions of joints and body segments
• Force, movement and power at each joint
• Activity of muscles while walking
• Pressure distribution on the feet to measure walking energy expenditure

Spastic Hemiplegia/Unilateral Gait Patterns
Spastic Hemiplegia is caused by damage to the motor cortex on one side of the brain brain which controls voluntary movement on the opposite side of the body. This type of Cerebral Palsy is marked by increased muscle tone or stiff muscles and spasticity, on one side of the body.
In spastic hemiplegia, four common gait patterns have been identified. These patterns build upon each other with impacting more muscle groups with increasing levels of muscle weakness, spasticity that act to create abnormal rotation and bone and joint deformities. It is important to identify each individual’s walking patterns as the management, interventions and treatments that are used are very different.
- Type 1 - Drop Foot
- Type 2 - Equinus
- Type 3 - Equinus / Jump Knee
- Type 4 - Equinus / Jump Knee / Stiff Gait
- Description - This gait pattern is characterized by weakness or the inability to lift the foot during the swing phase of gait.
- Treatment / Management - Often an orthotic will be used for management.
- Description - This is the most common gait pattern in Spastic Hemiplegia. It is characterized by toe walking, otherwise known as equinus.
It is caused by spasticity or contracture in the calf muscle and Achilles tendon. Within this gait type, there are two subcategories:
2A - Equinus (toe walking) with a neutral knee and extended hip
2B- Equinus (toe walking) with hyperextension knee and hip
Beginning in this gait pattern, the affected leg will be shorter.
-
Treatment / Management - Casting can be effective for mild contracture, tendon lengthening of the Achilles tendon can be helpful for fixed contractures to the gastroc-soleus (calf muscles) and orthotics are utilized to provide support, proper alignment and range of motion.
- Description - This gait pattern is marked by spasticity or contracture in the Achilles, calf muscles which impairs ankle flexion and a flexed stiff knee gait as the result of hamstrings and quadriceps contraction.
- Treatment/Management - An orthotic may be helpful for management and potentially a muscle tendon lengthening at the gastroc-soleus (calf muscle/Achilles tendon) if there is a contracture.
- Description - This gait pattern is characterized by spasticity or contracture in the Achilles, calf muscles which impairs ankle flexion and a flexed stiff knee gait as the result of hamstrings and quadriceps contraction plus hip adduction and internal rotation at the hip.
The person will be asymmetrical, one side of their body will clearly look different from the other.
-
Treatment / Management -
Treatment involves use of an orthotic, physical therapy, botulinum toxin, tendon and muscle tendon lengthening.
**While hip subluxation is rare in people with hemiplegia those with Type 4 and involvement at the hip should be under routine surveillance

Spastic Diplegia/Bilateral Cerebral palsy
Bilateral Spastic Cerebral Palsy is caused by damage to both sides of brain in the motor cortex to neurons that control voluntary movement of the lower limbs of the body. Individuals will have spasticity, muscle stiffness, primarily in both legs with the arms minimally impacted. This is the most common type of cerebral palsy.
As with hemiplegic cerebral palsy, there are also four commonly observed types of gait patterns which impact a person’s walking ability.
- Description - This gait pattern is characterized by toe walking due to spasticity in the calf muscles which causes the ankle joint to pull the heel up throughout the gait cycle with the hips and knees extended straight. Often the individual can stand with their feet flat on the floor with their knees hyperextended.
- Treatment / Management - An orthotic, muscle and/or tendon lengthening, physical therapy, and in some cases neurosurgery.
- Description - A common gait pattern in individuals with diplegia and includes spasticity in the calf muscles, hamstrings, and hip flexors. The ankle is in equinus, causing toe walking, the hips and knees are flexed and the pelvis is rotated forward causing a sway back. Often the individual will have a “stiff knee” because the of delayed or reduced knee flexing during the swing phase of gait. This type of gait pattern has a jumping appearance.
- Treatment / Management - PT, botulinum toxin, orthotics, muscle-tendon lengthening, and tendon transfer, hip / femur osteotomy and neurosurgery are all part of the toolkit to treat this gait pattern.
- Description - This pattern is involves more normal range of motion at the ankle, however the knee and hip are flexed through the stance phase of the pattern. Often it will appear that the individual is toe walking due to excessive flexing at the hip and knee and not due to pointing at the ankle.
- Treatment / Management - Treatment can include use of an orthotic, spasticity treatment such as botulinum toxin and/or muscle tendon lengthening.
- Description - This pattern is common in those with more significant spastic diplegia and most people with spastic quadriplegia who walk. It is recognized by excessive dorsiflexion at the ankle in combination with excessive bending at the knee and hip joints, as well as scissoring.
- Treatment / Management - Often a combination of treatments are used to help improve function with this pattern including lengthening of the hamstring and iliopsoas, a muscle deep in the hip, as well as correcting problems that arise with the bones in the legs and feet. Casting, orthotics, and PT are all utilized as well.
Less Common Gait pATTERNS IN CEREBRAL PALSY
Dyskinetic Cerebral Palsy: This form of cerebral palsy has several types of movement disorders characterized by involuntary, uncontrolled, recurring movement patterns and postures. Damage to the basil ganglia is attributed to the dyskinetic forms of cerebral palsy and impact involuntary movement in all four limbs.
Ataxic Cerebral Palsy: This is the least common type CP. Caused by damage, malformation to the cerebellum and/or genetic mutation, the movement disorder, ataxia, affects balance which leads to an unsteady gait and difficulties with balance and stability and impacts all four limbs.
- Description - This gait pattern is a type of dyskinetic cerebral palsy which is characterized by chaotic, jerky, uncontrolled movements usually in the hands, fingers and ankles.
- Treatment / Management - Treatment primarily includes medications and interventions such as PT, orthotics, bracing and devices to help manage the abnormal movements patterns and help the individual learn to compensate for them.
- Description - Balance is affected which leads to an unsteady gait and difficulties with balance and stability and impacts all four limbs. Often the individual walks with a wide gait.
- Treatment / Management - Interventions such as PT, orthotics and devices help individuals manage their condition and learn strategies to compensate for and improve balance and stability.
-

Gillette Children's