This systematic review looks at all available evidence for pharmacological/neurosurgical interventions for managing dystonia in individuals with cerebral palsy to inform the AACPDM care pathway.
We got the diagnosis of Cerebral Palsy when Lelia was 18 months. I was really happy, as we didn’t know what was wrong with her before then. She had low tone. She couldn’t roll over. She couldn’t sit up. Of course she didn’t walk. The diagnosis gave it a name, something I could work with, and I became a kind of vigilante mother, determined to get the best care for my daughter.

Spasticity is usually caused by central nervous system injuries, such as brain injuries or spinal cord injuries. Spasticity is a little different from stiffness.
There are so many different causes for potential pain that it can be hard to find the cause. If you have CP or are a parent of someone with CP it is really important to empower yourself with information on pain including what causes it and options for treatment. You need to work out what is causing the pain not just mask it with pain medication.

When we have a physical disability, our bones can get a bit weak or osteoporotic. Something that can be improved is promoting bone health for people with cerebral palsy.

It is important to understand the brain injury for each individual person, because they can be really different. Where the injury is can give us important clues to what motor problems that individual will have. The time you have the biggest risk to having a stroke is as a baby, not as an adult so it is important to understand what may be happening in the infants brain.
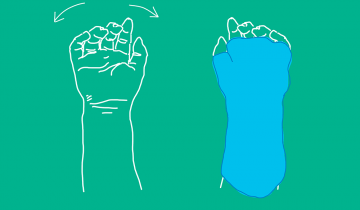
Upper limb therapies and interventions have been well studied in cerebral palsy. Different interventions that have good evidence are Constraint Induced Movement Therapy (CIMT) and Bimanual Therapy. CIMT has been shown to be successful in children with hemiplegic cerebral palsy (CP). CIMT uses a splint to physically constrain the uninvolved arm and encourage them to use the more involved or affected arm.